발성훈련 기능성 게임 개발을 위한 기능성 게임 및 이해당사자 요구 분석
An Analysis on Serious Games and Stakeholders' Needs for Vocal Training Game Development
Article information

Abstract
배경 및 목적
본 연구는 발성훈련에 대한 언어치료 환자의 치료 동기와 참여를 향상시키기 위한 기능성 게임에 대한 요구사항과 개발방향을 파악하기 위해 수행되었다.
방법
문헌조사, 이해당사자 요구조사, 기존 3가지 발성훈련 게임(Visi Pitch, Dr. Speech, Vox Sys-tem)의 벤치마킹 분석이 수행되었다.
결과
문헌조사를 통해 13가지 게임 사용자 경험 척도들(유용성, 서사성, 몰입, 즐거움, 창의성, 오디오 심미성, 개인적 충족감, 사회적 연결성, 시각적 심미성, 정확성, 개인 맞춤형 분석, 게임 분석, 치료 연속성)이 파악되었다. 사용자 경험 척도들 중 기존 언어치료게임에서 일반적으로 미흡한 속성들로는 창의성(평균 만족도= 2.5–4.3; Likert 7점 척도 사용), 사회적 연결성(2.4–4.4), 치료 연속성(1.7–4.7), 그리고 개인 맞춤형(2.5–5.0)이 파악되었다.
논의 및 결론
본 연구의 사용자 경험 척도들은 발성훈련 기능성 게임을 평가하는 데 유용하게 활용될 수 있으며, 기존의 게임들이 상대적으로 미흡한 사용성 경험 척도를 보완하는 새로운 기능성 게임 개발이 필요하다.
Trans Abstract
Objectives
The present study intended to identify the needs and development directions of a serious vocal training game for better motivation and commitment of patients with voice disorder to voice therapy.
Methods
A literature review, a survey of stakeholders' needs, and a benchmarking analysis of three vocal training games (Visi Pitch, Dr. Speech, and Vox System) was conducted.
Results
From the literature review, thirteen game user experience scales (usability, narratives, play engrossment, enjoyment, creative freedom, audio aesthetics, personal gratification, social connectivity, visual aesthetics, accuracy, customization, game analytics, and therapy continuity) were identified for vocal training games and then applied to evaluation of the existing games. From the user experience scales, features not commonly implemented in the existing games include creative freedom (average satisfaction score, 2.5 to 4.3 out of 7), social connectivity (2.4 to 4.4), therapy continuity (1.7 to 4.7), and customization (2.5 to 5.0).
Conclusion
The user experience scales would be of use to assess vocal training games, and new serious games need to be developed to complement the existing games in terms of the four scales found relatively lacking.
Voice disorders are characterized by the abnormality of pitch, loudness, quality of sound, and/or duration in voice production; resulting in a significant need of therapy (Ziegler & Hapner, 2013). The estimated prevalence of voice disorders among US young adults aged 24–34 years is 6% (Bainbridge, Roy, Losonczy, Hoffman, & Cohen, 2017), and that among US children aged 3–17 years is 1.4% (Black, Vahratian, & Hoffman, 2015). However, the percentage of patients with voice disorders seeking treatment is 0.98% (Cohen, Kim, Roy, Asche, & Courey, 2012), indicating most individuals with voice disorders do not receive treatment. Among the treatment-seeking population, the prevalence of voice disorders is reported to be higher in female adults than male adults, with an odds ratio of 1.5 (Martins et al., 2016; Roy, Merrill, Gray, & Smith, 2005), male children than female children (Carding, Roulstone, & Northstone, 2006; Martins et al., 2016), and elderly adults (4.8%-29.1%) than children (1.4%-6%) (de Araújo Pernambuco, Espelt, Balata, & de Lima, 2015).
Voice therapy can help patients with voice disorders acquire self-confidence, independence, and social skills by improving their voice production. Voice therapy is conducted for the training of voice production in controlling voice tone (pitch), intensity (loud-ness), and breath (continuity) (Saz, Yin, Lleida, & Rose, 2009). Con-ventionally, voice therapy is conducted based on mechanization (Navarro-Newball et al., 2014) and therefore it is hard to maintain a patient’ s motivation and attention during the therapy session, unavailable at home, and limited by the subjective evaluation of a therapist.
Serious games can be an effective assistance in voice therapy by motivating patients with voice disorders through the accomplishment of fun tasks. Serious games have been developed for purposes more than mere entertainment and increasingly applied in edu-cation, training, and healthcare; for example, some healthcare purposes of serious games include health monitoring, diagnosis, treatment, therapy, and rehabilitation (Wattanasoontorn, Boada, García, & Sbert, 2013). Therapists and patients have provided positive responses to the application of serious games to speech therapy (Grossinho, Cavaco, & Magalhães, 2014; Navarro-Newball et al., 2014; Vicsi, 1995). Examples of speech therapy games include Articulation Station (Little Bee Speech, USA), Dr. Speech (Batalla et al., 2014), Speech Mirror (CluSoft, Seoul, Korea), Talking to Teo (Navarro-Newball et al., 2014), Visi-Pitch (Perry, Ingrisano, & Scott, 1996), and Vox System (RS Care Systems, Daegu, Korea). Shtern, Haworth, Yunusova, Baljko, and Faloutsos (2012) reported that serious games increased patients' motivation and sustainment in speech therapy compared with the conventional therapy by providing immediate feedback and intuitive gaming scenarios. Furthermore, it is reported that the majority (78%) of patients treated for speech therapy were children aged 12 or under (Pyo, 2013) and the majority (97%) of speech therapy treatments with children patients are practiced in clinical environments (Choi, 2013). Though the number of commercial serious games has been incre-asing, the percentage of speech therapy-related games among all serious games is 0.93% (Wattanasoontorn et al., 2013), indicating the needs of developing more serious games for speech therapy.
An integration of emerging technologies, including smart devices and virtual reality technologies, with conventional speech therapy programs has been explored with careful considerations. Kim et al. (2017) and Lee, Park, and Yoo (2019) developed smartphone based programs for the continuity of voice therapy from clinical to reallife environments. Da Silva, Fernandes, and Grohmann (2015) proposed an augmented reality based interactive system which assists interventions with children with autism spectrum disorders performed by speech therapists and supports par-ents' participation in the interventions. Kim and Kwon (2018), Kim, Kwon, Kwon, and Paeng, (2019), and Park, Kim, Lee, Bae, and Kwon (2019) examined the effects of augmented reality based language therapy programs on the intervention of children with language disabilities. Evidence of the transfer of functional communication skills acquired during virtual environments to realworld situations supports the potential of the emerging technologies of the fourth industrial revolution era in the field of speech-language pathology. However, safety and ethical issues such as cyber sickness and cyber security need to be carefully considered during the research and practice of virtual reality technologies (Bryant, Brunner, & Hemsley, 2019).
The present study intended to identify the needs and development directions of a vocal training game to better support voice therapy through a systematic analysis of stakeholders' needs and existing games. Game user experience scales were identified by a literature review and then a questionnaire was prepared based on the identified game user experience scales for the evaluation of vocal training games. Game user experience scales lacking in the existing games were identified and a benchmarking of existing games was performed to identify key features to be applied to new serious game development.
METHODS
Identification of Game User Experience Scales
A literature review was conducted to identify user experience scales for evaluation of vocal training games. Articles of serious games for speech therapy were systematically searched by keywords including ‘speech therapy’ and ‘serious game’ and screened by title, abstract, and content, resulting in 13 articles for review.
Benchmarking of Existing Vocal Training Games
Several commercial serious games such as Visi Pitch (Pentax Medical, Montvale, NJ, USA), Dr. Speech (TigerDRS Inc., Seattle, WA, USA), and Vox Systems (RS Care Systems, Daegu, Korea) providing vocal training functions are available on the market. These three games are often used by clinicians and therapists as a supporting tool for conducting voice therapy. Their weaknesses and strengths were analysed to identify key features applicable to vocal training game development.
Survey of Stakeholders'Needs
A questionnaire survey was conducted to analyze the needs of stakeholders for vocal training games. Eighteen speech therapists (6 males and 12 females) having over 3 years of experience in voice therapy participated in the survey. The percentage of speech therapists who had used serious games for voice therapy for more than one year and that of the therapists who had used serious games for voice therapy more than once a week were 77.2% and 66.7%, re-spectively. As for vocal training games the therapists found most effective based on their experience, Visi Pitch was selected most highly (42.1%), followed by Dr. Speech (26.3%) and Vox Systems (5.3%). Lastly, children under the age of 12 years were found dominant (77.8%) among the patients the therapists had provided for vocal training services.
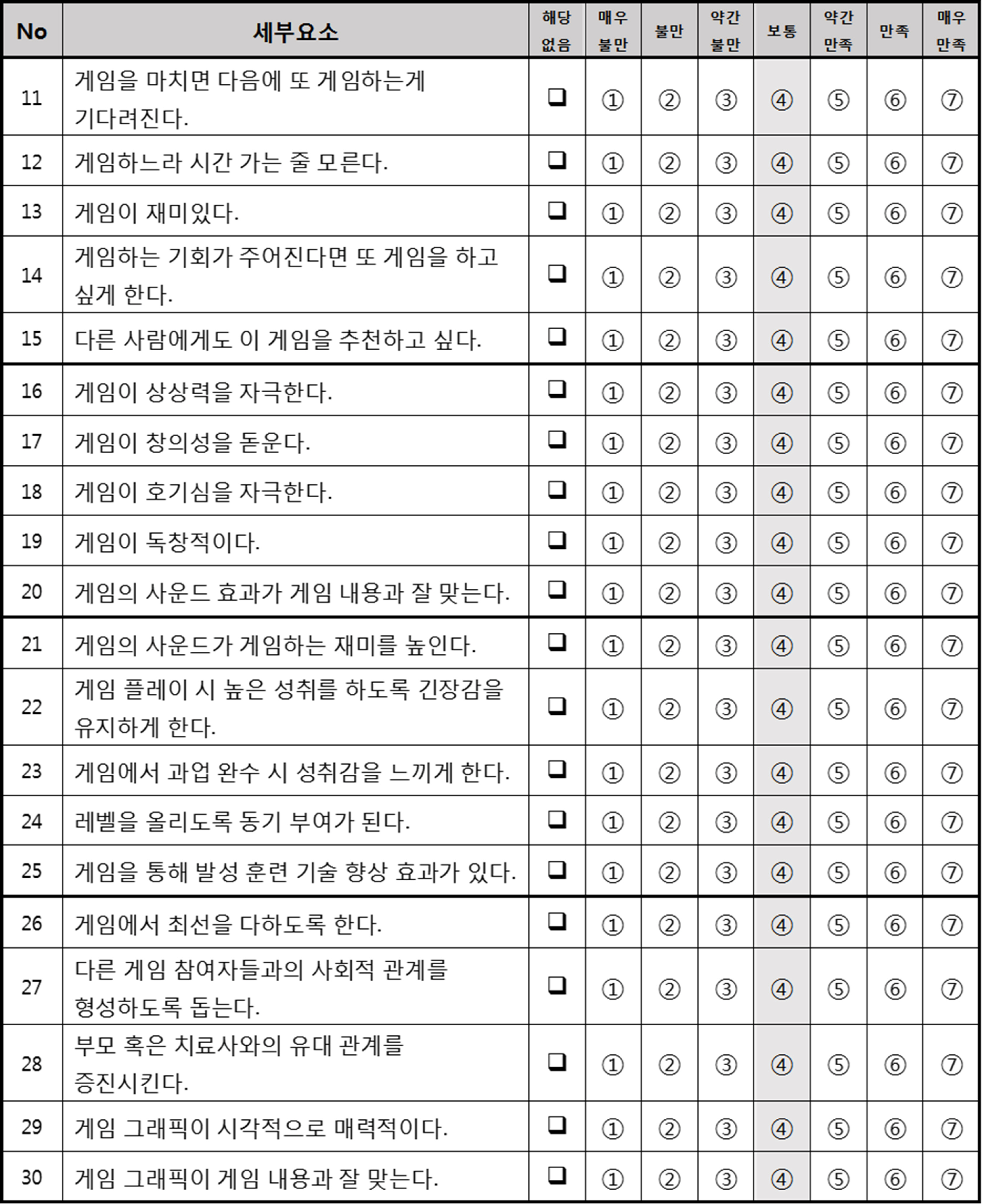
The questionnaire in Appendix 1 consisting of 36 statements for 13 game user experience scales, with a 7-point Likert scale (‘1’ for very dissatisfied and ‘7’ for very satisfied), was used for speech therapists to evaluate a vocal training game that they had selected as most effective in vocal therapy based on their experience. The average satisfaction scores was calculated for each user experience scale by referring to Table 1. User experience scales which were commonly lacking in existing vocal training games were identified from the survey evaluation results. In addition to the thera-pists' experience with the vocal training games, likes, dislikes, and suggestions for each game were surveyed. Patients with voice disorders and their guardians were not included in the survey due to their limited experience in voice therapy games. The research protocol of the present study was approved by the Institutional Review Board at Pohang University of Science and Technology (No. PIRB-2016-E044).

Game user experience scales
RESULTS
Game User Experience Scales
A total of 13 scales presented in Table 1 were identified based on the review of 13 articles as those needed for the user experience attributes of vocal training games. Nine game user experience scales including usability, narratives, play engrossment, enjoyment, creative freedom, audio aesthetics, personal gratification, social con-nectivity, and visual aesthetics were adopted from the Game User Experience Satisfaction Scale (GUESS; Phan, Keebler, & Chapar-ro, 2016). In addition to the nine GUESS scales, four scales including accuracy, customization, game analytics, and therapy continuity were added based on the review of the other articles (Cagatay, Ege, Tokdemir, & Cagiltay, 2012; Faria et al., 2014; Grossinho et al., 2014; King, Davis, Lehman, & Ruddy, 2012; Kostoulas et al., 2012; Lee, Kim, Yoo, & Ko, 2015; Marache-Francisco & Brangier 2016; Mayer, 2012; Navarro-Newball et al., 2014; Shtern et al., 2012; Vicsi, 1995; Wattanasoontorn et al., 2013). The statement numbers in Appendix 1 corresponding to each of the user experience scales are indicated in the last column of Table 1; the first 30 statements were adopted from the GUESS study by Phan et al. (2016) and the remaining 6 statements were prepared for the four newly added scales and by referring to related papers.
Benchmarking of Existing Vocal Training Games
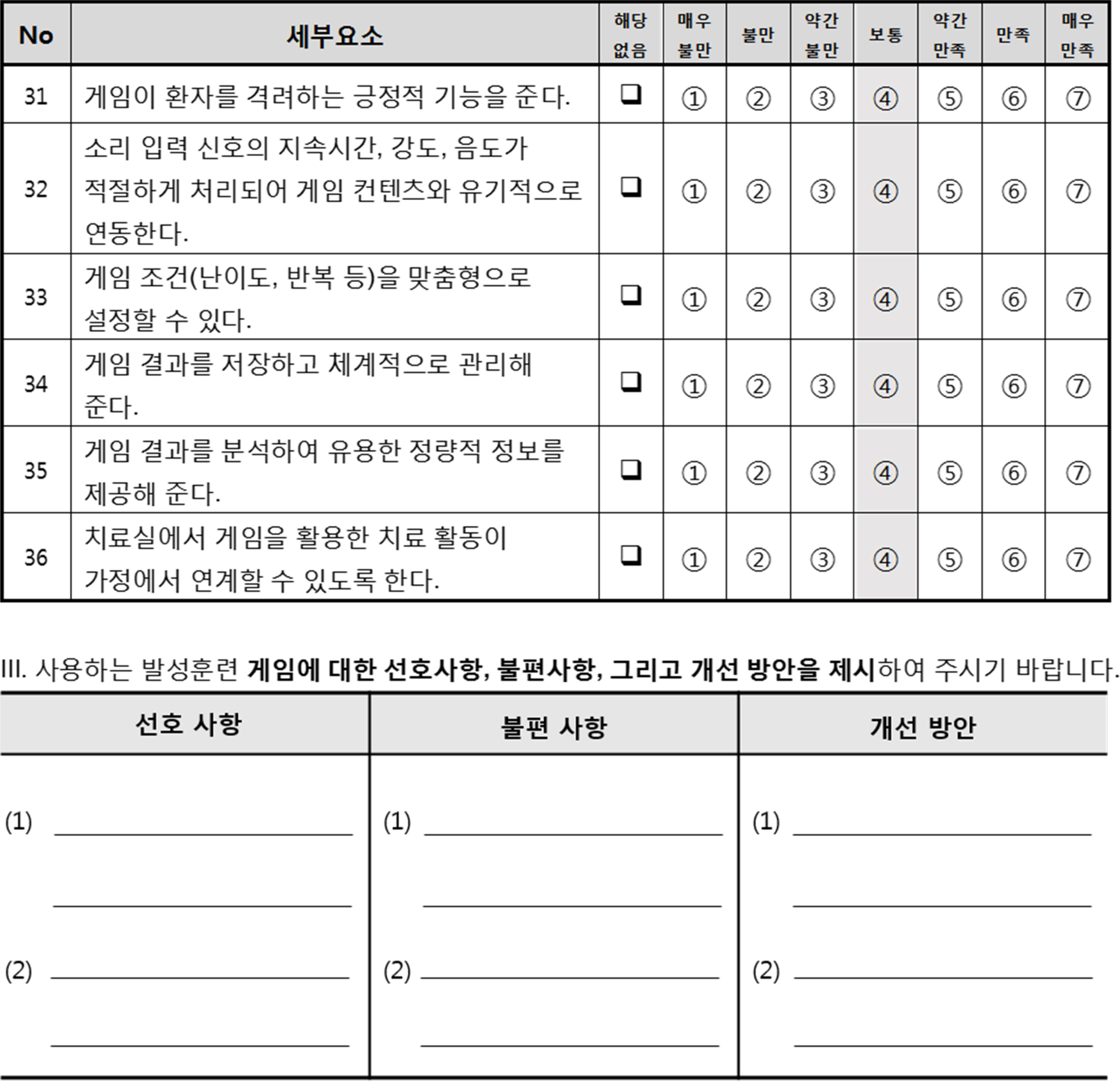
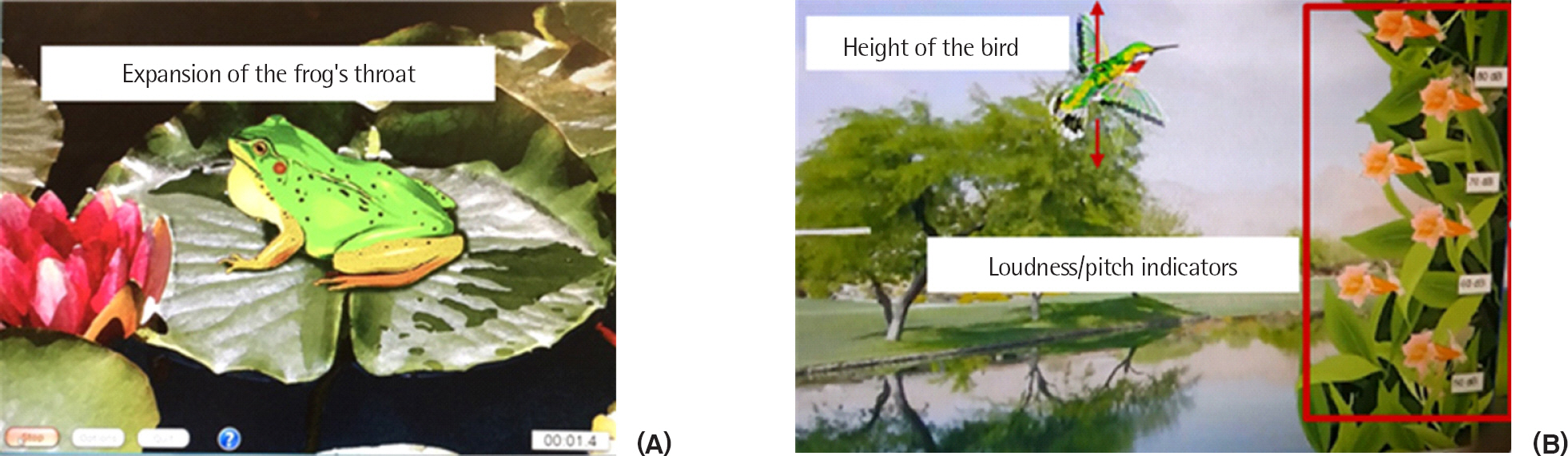
Three vocal training games including Visi Pitch, Dr. Speech, and Vox System were compared to identify key features applicable to the development of a vocal training game with better features. Of the existing vocal training games, these three vocal training games were selected as most effective by the therapists in the survey of the present study by a relatively high margin. All the vocal training games provide the training functions of voice production in vocal continuity, loudness, and pitch; and allow therapists to set the target level, training time, and repetition of vocal continuity, loudness, or pitch according to therapeutic needs for a particular patient with a voice disorder. For example, for the training of vocal continuity in Visi Pitch, a patient needs to produce a continuous voice to expand a frog’ s throat until the frog croaks to collect the frog (Figure 1A) and then repeat the task until he or she collects the required number of frogs. For the training of pitch or loudness in Visi Pitch, a patient needs to produce a voice at different levels of pitch or loudness to control a bird to fly to the flowers at different heights (Figure 1B); and then visual feedback, such as size of the frog’ s throat and height of the bird, is provided in real time so that the patient can maintain his or her voice at a certain level of vocal continuity, loudness, or pitch. The recording and plotting functions of a patient’ s vocal production time, loudness level, and pitch level during the gameplay in Dr. Speech provide quantitative analysis of a patient’ s performance for therapists as shown in Figure 2. Vox Systems provides a more advanced vocal continuity training function in which a patient needs not only to produce a continuous voice to allow a game character to cross a street, but also stop voice production to freeze the character if a car randomly passes through as shown in Figure 3. All the features aforementioned are found desirable to the development of a new vocal training game.
Vocal training games in Visi Pitch: (A) frog game for vocal continuity training and (B) bird game for vocal loudness/pitch training.
Vocal training games in Dr. Speech: (A) boat game for pitch training and (B) cat rescue game for loudness training with game play time, pitch levels and loudness levels recorded and plotted.

Street crossing game for vocal continuity training in Vox Systems.
Survey of Stakeholder's Needs
As displayed in Figure 4, the stakeholders' needs survey results indicate that a new vocal training game needs to pay more attention to four (creative freedom, social connectivity, therapy conti-nuity, and customization) user experience scales. Of the game user experience scales, creative freedom (average satisfaction score, 2.5 to 4.3 out of 7), social connectivity (2.4 to 4.4), customization (2.5 to 5.0), and therapy continuity (1.7 to 4.7) were found relatively lacking in the three existing games. Furthermore, the therapists suggested providing more games in Vox Systems to keep patients from becoming tired or bored, various difficulty levels in Dr. Speech to maintain patients' motivation, and improving Visi Pitch with modern graphic designs.
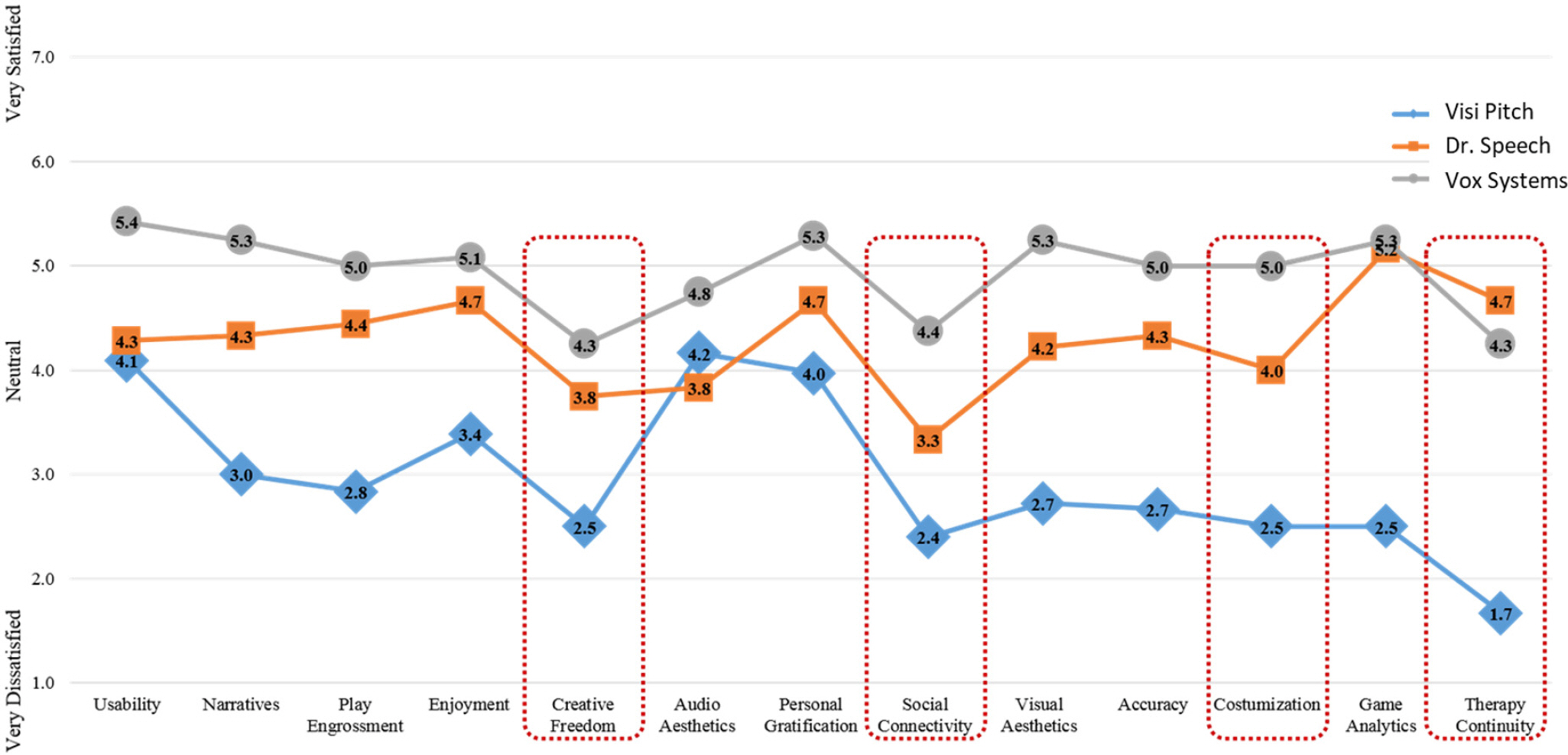
Game user experience satisfaction scores for Visi Pitch, Dr. Speech, and Vox Systems. Game user experience scales which were not commonly satisfied in the three games were indicated by a dotted box.
Directions for Serious Game Development
Detailed features of each scale applicable to vocal training game development are summarized in Table 2. For example, for the scale of social connectivity, a new game needs to provide interaction functions with other players and facilitators (e.g., therapist, par-ents, and caretakers) by providing a multiplayer module in the game for interaction with other players to build social skills for patients.

Features of game user experience scales for voice therapy game development
DISCUSSION & CONCLUSION
Thirteen game user experience scales for evaluation of vocal training games were identified based on a literature review. Among the identified scales, nine scales (usability, narratives, play engrossment, enjoyment, creative freedom, audio aesthetics, personal gratification, social connectivity, and visual aesthetics) were adopted from GUESS (Phan et al., 2016) and the four scales (accura-cy, customization, game analytics, and therapy continuity) were identified from the review of the other papers to complement the GUESS scales. The game user epxerience scales can be asserted to have content validity because they were extracted from the papers demonstrating their content validity (Phan et al., 2016) and/or corresponding to vocal training games, and they were effectively applied in the present study to the satisfaction evalaution of the vocie training games.
Features applicable to vocal training games were effectively identified in the present study through the benchmarking of the three existing speech training games, including Visi Pitch, Dr. Speech, and Vox Systems. First, vocal training games need to cover the training of vocal continuity, loudness, and pitch. Second, customized difficulty levels, including a target level, training time, and repetition times of vocal continuity, loudness, or pitch can be set in the games according to patients' therapy needs. Third, visual feedback indicating the levels of patients' vocal continuity, loudness or pitch is needed in real time; especially for children having difficulties in recognition of their own voice (Pyo, 2013), so that patients can maintain their voice around the target levels to accomplish game tasks. Fourth, recording and plotting functions of patients' vocal production time, loudness and pitch levels during gameplay can be used for quantitative analysis of patients' performance in vocal production. Lastly, game scenarios need to be designed to provide the vocal training of patients at different therapy stages with different disorder levels. For example, a simple game can be provided for a patient at the beginning stage of therapy and then gradually more difficult games can be used for the patient as his or her capability increases.
Game user experience scales which were not commonly implemented in the three existing games were identified through stake-holders' needs survey. Therapists provided relatively low satisfaction scores to the existing games in creative freedom (average satisfaction score, 2.5 to 4.3), social connectivity (2.4 to 4.4), therapy continuity (1.7 to 4.7), and customization (2.5 to 5.0). In particular, they suggested providing games with different scenarios, stories, difficulty levels, and modern graphic designs to maintain patients' motivation, fun, and commitment for better effectiveness of voice therapy games.
Vocal training games need to be developed by applying the features for each of the 13 game user experience scales summarized in Table 2. For example, for therapy continuity, a therapist’ s system at a clinic and a patient’ s system at home need to be integrated via a cloud-based system so that the patient can continue vocal training at home after clinical therapy by accomplishing tasks that the therapist assigned online.
New serious games for vocal training need to be developed based on the identified stakeholder’ s needs and the development directions in the present study. Figure 5A shows examples of new games for continuity, loudness, and pitch training and Figure 5B illustrates a seesaw game requiring a patient to imitate the loudness level of a therapist for better social connectivity. New games can be evaluated using the questionnaire established in the present study to compare with the existing games. Furthermore, the identified 13 game user experience scales and the survey of stakeholders' needs can be used for needs analysis and development directions establishment of general serious games. Advanced vocal training serious games need to be implemented as smart device applications and mobile-based contents in the convergence era of information and communication technologies to better satisfy the needs of speech-language pathologists and parents in speech-language intervention for children with communication disorders (Lee, Kim, & Park, 2016; Yim, Kim, Park, Cheon, & Lee, 2014).

Examples of new vocal training games: (A) games for continuity, loudness, and pitch training, and (B) a seesaw game requiring a social interaction be- tween a therapist and a patient.
Lastly, the stakeholder’s needs and development directions identified in the present study can be considered in the evaluation of vocal therapy programs based on emerging technologies. Studies including da Silva et al. (2015), Kim and Kwon (2018), Kim et al. (2017), Kim et al. (2019), Lee et al. (2019), and Park et al. (2019) have applied smart devices and virtual reality technologies to assessment and intervention in speech-language pathology. Voice therapy systems based on emerging technologies can be evaluated in terms of the stakeholder’ s needs identified in the present study and directions of improvement for the advanced technology based systems can be effectively proposed.