

Humor is not only present in the lives of older people but is beneficial to their well-being and serves as a coping mechanism for aging (Damianakis & Marziali, 2011). Moreover, it has an important social dimension for the elderly as it improves relationships (Richman, 1995; Damianakis & Marziali, 2011). However, understanding of humor can be affected by aging (Shammi & Stuss, 2003) or age-related psychiatric disorders such as dementia (Clark et al., 2015) and depression (Samson, 2014; Uekermann et al., 2008). Studies on humor processing in depressed adults and in people with dementia show that understanding humor depends both on the type/severity of the disease and the type of humor (Clark et al., 2015; Shammi & Stuss, 1999; Uekermann et al., 2008). Apart from a study by Walter et al. (2007) that compares the effects of humor therapy comparing the depressed elderly and those with dementia, the relationship between humor and those two disorders is rarely discussed. Since dementia and depression are common (Leyhe et al., 2017; Valkanova, Ebmeier, & Allan, 2017; WHO, 2017), often correlated or hard to distinguish problems in old age (Leyhe et al., 2017; Steffens & Potter, 2008; Steinberg & Rosenberg, 2017), it is worth investigating how they affect humor processing and appreciation. It is especially important since humor can be a useful diagnostic tool in a psychiatric assessment (Goldin & Bordan, 1999; Sultanoff, 2003) as well as in a neurodegenerative assessment (Clark et al., 2015; Sivasathiaseelan et al., 2021). This study aims to explore humor preferences in the elderly participants with dementia or/and depression and establish how those particular disorders influence the perceived funniness of more and less cognitively challenging verbal jokes of different types.
Humor Processing
Humor processing is a complex task that requires both cognitive and emotional aspects that influence mental operations underlying humor comprehension (Willinger et al., 2017). Thus, on the one hand humor is an intellectual challenge, and on the other hand it depends on the mood and thus affective components (Vtricka, Black, & Reiss, 2013).
Humor preferences that are the subject of our paper are not synonymous with humor comprehension but are closely related. Humor preferences give us an insight into what a person enjoys, and we may assume that to enjoy (appreciate) humor a person needs to understand a joke. Humor processing comprises two stages: comprehension being the first stage and appreciation being the second stage (Aykan & Nalçacı, 2018).
Craik and Ware (2007) explain that humor comprehension is the ability to understand humor and humor appreciation is the disposition to enjoy and react to humor. However, research into the humor of the elderly shows that humor may be appreciated even if not fully understood (e.g., Shammi & Stuss, 2003).
In terms of humor understanding, different types of humor require more or less cognitive effort. Non-verbal humor such as slapstick is much simpler than verbal humor that requires mentalizing skills which are more cognitively demanding (Dunbar, Launay, & Curry, 2016). It does not mean however that all verbal humor is difficult. For instance, children’s jokes often rely on simple incongruities, norm violations or errors (McGhee, 2002; SemrudClikeman & Glass, 2010) whereas with age we learn to understand and enjoy more complex humor such as irony, sarcasm (Martin, 2007) or metaphors (Hoicka, 2014). According to Schaier and Cicirelli (1976) as we get older both our cognitive ability and humor comprehension decline, which leads to an increased appreciation of the humor as the joke requires more cognitive effort from the individual.
According to Hoicka (2014) early humor is relatively simple. Children’s humor points only to literal ambiguity, or wrongness of the act, paired with the intention to amuse (Hoicka & Gattis, 2008). However, adult humor can also be simple. In general, puns or plays on words, which often rely on some kind of linguistic error, represent one of the simplest forms of jokes, often on the verge of not being funny (Ritchie, 2004). Most universally appreciated examples of humor are those that are simple, highly visual and in tune with the basics of innate or more primal levels of human common sense (Reimann, 2010, p. 25).
Understanding pretense, irony, and metaphor is more complex (Hoicka, 2014). According to Steen (2018) comprehending metaphor is a cognitively demanding puzzle that requires making sense of the inconsistent correlation of two conceptual domains that are linguistically associated but not directly related to each other. It could be argued that understanding metaphor-based jokes is more difficult than error-based jokes that merely require noticing the error (the difference) and knowing what is correct or expected. However, any type of joke, including metaphor-based jokes can be familiar/well-known to the audience. This leads to a question of whether familiarity makes humor simpler to understand.
The salience hypothesis proposed by Suls (1972) assumes that if the joke content is relevant to the individual, he will find it funnier than a non-involved individual. Heightened salience may enable people to process humor stimuli more easily and ‘get’ related types of humor more readily (Goldstein, Suls, & Anthony, 1972).
According to Triezenberg (2004) knowing exactly what is going on and how things are going to work also inflates the reader’s self-confidence, making it more likely that he/she will understand sophisticated jokes.
As for humor appreciation, familiarity plays an important role in enjoying humor. According to Suls (1975) we both find familiar and novel humor funny but for different reasons. We enjoy the former because of the sense of satisfaction when remembering the joke and the latter because of the satisfaction from the surprise provoked by the incongruity. Repetition is inherently funny in itself and humor in it can derive from, among others, the fact that the audience knows what is coming (Triezenberg, 2004). This contrasts with the idea that simple and familiar jokes are not funny because they do not represent moderate novelty and complexity that help us maximally enjoy humor (Weisfeld, 2019). Goldstein (1970) claims that repeated exposure to a joke may lessen the tension caused by its novelty and thus make a person enjoy it more. Lessening the novelty-driven tension may be especially important for dementia patients for whom familiarity is crucial. According to Son, Therrien, and Whall (2002) a familiar environment is important for daily life in cognitively impaired elders, introducing the sense of familiarity into a new or strange environment as well as maximizing familiarity in an existing environment. Therefore, they argue, new interventions should be focused on using aspects of prior familiar environments such as smells, music, foods, or objects and pictures in order to maximize functional ability in elders with dementia. This possibly concerns humor too.
Not just familiarity but also identification is important for humor appreciation. To find something funny we generally need to identify with it, which means having an underlying sympathy with the viewpoint of the humorist and/or understanding of a person or situation (Holland, 1982; Plester & Inkson, 2019) or sharing a familiar reference (Libera, 2020). The study by Lynch (2010) shows that people laugh more in response to specific bits which match their implicit preferences, meaning that we find something funny because we think it is true.
The challenge of understanding and appreciating humor also lies in its culture and context-dependent nature. Humor does not happen in the void but is borne within a social context (Martin, 2007) and thus even one misinterpreted element may deem humor incomprehensible.
When talking about humor processing, we also need to take into account aging and the diseases that may affect an older person’s understanding or/and appreciation of humor thus humor preferences.
Humor in the Healthy Elderly
The study by Proyer, Ruch, and Müller (2010) shows that age does not seem to have a major impact on playfulness or on the sense of humor; both remain stable over the age span. The study also reveals that positive mood increases with age, however, the older people laugh less often and less easily. What is more, the study argues that humor may depend on how often the elderly socialize - the more often they spend with their friends, the higher their playfulness and positive mood level. Similar to Proyer et al. (2010), the study by Greengross (2013) shows the amount of laughter exhibited by the elderly is smaller compared to young adults. In addition, he notes that the older population seems not to enjoy aggressive types of humor as much as the younger ones, and the elderly are especially sensitive to jokes referring to old age. According to Shammi and Stuss (2003) aging affects cognitive comprehension of humor but does not affect emotional responses to humor. They suggest that the preserved affective responsiveness may underlie the success in using humor as a coping mechanism in the elderly. Thorson and Powell (1996) note that there is some evidence suggesting that elderly people tend to use humor as a coping mechanism more often than the younger population. For example, Schiau (2016) shows that older women tend to use humor in interpersonal situations and that there is a significant correlation between the use of this type of humor and a reduced sense of social loneliness.
Biscetti, Ceccato, Lecce, Cavallini, and Bambini (2019) argue that humor comprehension among healthy older adults also depends on the type of humor. Their study reveals that older adults find mental jokes more difficult than phonological jokes. The former require greater cognitive effort, i.e., reasoning about mental states of the characters in the joke, whereas the latter are easier to understand as their funniness lies in the similar sounds representing puns. Shammi and Stuss (2003) also note that cognitive complexity is a factor influencing humor comprehension in normal ageing. The elderly in their study did not differ from young participants in terms of simply assigning humorous items to stimulus items but they struggled with more complex tasks of joke stem completion and cartoon selection.
Humor in Depression and Dementia
Humor, being a complex phenomenon, relies among others on cognition and emotions (Clark et al., 2015; Martin, 2007; McCreaddie & Wiggins, 2009; Shammi & Stuss, 2003). Two common elderly diseases, i.e., depression and dementia (Valcanova et al., 2017), can affect both emotions and cognition (Steffens & Potter, 2008) necessary for appreciating humor (Vrticka, Black, Neely, Walter Shelly, & Reiss, 2013) and creating and understanding humor (Greengross, 2013). However, it has been shown that depression affects not only appreciation of humor (affective aspect) but also its comprehension of cognitive processes (Samson, 2014; Uekermann et al., 2008). Similarly, dementia not only affects humor cognition but also the emotional response. The right frontal damage, observed in dementia, not only causes an impairment in humor cognition but also in emotional responses to humorous stimuli (Shammi & Stuss, 1999; Sivasathiaseelan et al., 2021).
Generally, depression is associated with mood changes which inhibit enjoyment of humor (Forabosco, 1998). Humor and mood represent a two-tier relationship as our mood influences our enjoyment of humor (Forabosco, 1998; Willinger et al., 2017) and conversely humor influences our mood (Szabo, 2003; Wellenzhohn, Proyer, & Ruch, 2018; Zhao et al., 2019).
However, laughter and sense of humor can be used to camouflage a low mood/depression (Atkinson, 2011). One problem with detecting depression in the elderly is that older persons may be more successful than their younger counterparts at masking or hiding symptoms of depression (Hooyman & Kiyak, 2008). Kortbein and Means (2012) show that elderly persons minimize their depressed mood to others. According to Neville and Byrne (2009) it is not uncommon for the depressed elderly to display superficial socially sanctioned smiles called ‘smiling depressive’. Similarly, Whall and Hoes-Gurevich (1999) show that the elderly use smiles to mask/hide depression.
In contrast, Bokarius’s et al. (2011) study on the correlation between disposition to humor and level of depression shows that older adults were the only ones with marginally significant negative correlation between Disposition Towards Humor (DTH) and depression. According to the authors, the older population may be less likely to accept humor in their treatment as a function of depression.
The existing studies on humor and depression do not specifically focus on the elderly humor preferences. Thus, humor in late life depression is an under-researched topic limited mainly to studies discussing the effectiveness of humor intervention/therapy on the well-being of the elderly.
A study by Walter et al. (2007) is the only study concerning the relationship between humor and both late-life depression and Alzheimer’s disease. It shows the improved quality of life, mood, depression score and instrumental activities of daily living for depressive patients in both humor therapy and standard therapy groups. The highest quality of life after humor therapy was found in the depressed patients without Alzheimer’s disease (AD). However, there was no significant effect of humor therapy compared with standard therapy; and patients with AD of both therapy groups did not significantly improve in terms of quality of life.
Other studies on the effects of humor therapy on the elderly do not concern seniors diagnosed with depression. However, they show an improvement on the geriatric depression scale after humor intervention (Brodaty et al., 2014; Zhao et al., 2019), which proves the elderly react to humor.
As for humor in dementia, humor being a complex cognitive and emotional construct is vulnerable to neurodegenerative diseases, notably frontotemporal lobar degeneration (Clark et al., 2015).
Observing spontaneous humor in cognitively impaired patients (CI), Saunders, de Medeiros, and Bartell (2011) noticed that CI patients used humor as often as non-CI patients. They distinguished different functions of humor used by CI patients, namely dominant/control humor, relational/solidarity building humor and selfdenigrating humor. The study shows that humor may be an assertive move by patients, reflecting a need to actively participate in discussions regarding their health.
Clark et al. (2015), Clark et al. (2016) and Shammi and Stuss (1999) on the other hand used pre-selected jokes. They found differences in humor processing based on a type of dementia and type of humor.
Clark et al. (2016) assessed humor behavior and preferences in patients with Alzheimer’s disease and syndromes of frontotemporal lobar degeneration (FTLD), namely behavioral variant frontotemporal dementia (bvFTD), semantic dementia (SD) also known as primary progressive aphasia - semantic variant (svPPA), and progressive non-fluent aphasia (PNFA) versus healthy individuals. Alzheimer’s disease is the most common cause of dementia in the elderly. BvFTD typically presents with changes in behavior, personality, and social behavior; while SD and PNFA present with language dysfunction. They have shown that dementia syndromes commonly produce an altered sense of humor, and this alteration differs qualitatively and quantitatively between dementia syndromes.
Altered humor was universal in bvFTD and SD, but occurred in a substantial minority of patients with PNFA and AD. Increased fatuity and relative predilection for childlike or slapstick humor and less pleasure in other comedy genres were features of all dementia syndromes, while frankly inappropriate humor in response to unpleasant or impersonal stimuli was a hallmark of bvFTD and SD. Moreover, development of abnormal humor expression correlated with executive impairment across syndromes and with clinical disease duration in AD, but not FTLD syndromes, supporting the clinical impression that sense of humor is often impoverished early in FTLD, but relatively preserved initially in AD.
Moreover, in another study Clark et al. (2015) used non-verbal humorous cartoons, some based on familiar incongruities (conventionally incongruous slapstick or farce stock elements) and others were novel incongruities based on incompatible beliefs or concepts that required an active perspective shift by the viewers. Patients with bvFTD had greater difficulty recognizing novel humor, whereas patients with SD had greater difficulty detecting familiar humor. The authors conclude that bvFTD is particularly associated with impaired detection of humor where it is based on the active deconstruction of a novel incongruous situation, while SD is a more general defect of humor detection that extends to familiar humorous scenarios. Clark et al. (2015) show that despite both types of dementia being associated with extensive abnormalities of humor processing, more fatuous and childlike humor may be a marker of bvFTD. The patients with bvFTD tended to over-label novel control cartoons as humorous, whereas patients with SD tended to reject familiar humorous cartoons as non-humorous.
Shammi and Stuss (1999) show that there is a difference between humor understanding in patients with left frontal lesions and posterior damage and those with the damage in the right frontal lobe. The former did not differ significantly from the control group in their ability to distinguish funny from neutral items in terms of assigning funny ratings, complete joke stems with appropriate punchlines, or in their reaction to humor stimuli. However, the latter impaired the patients’ ability to respond to humor and the performance of humor tests correlated with working memory, mental flexibility, and abstract reasoning.
Wong and Kumfor (2022) on the other hand show that patients with right temporal variant frontotemporal dementia (rtvFTD) may laugh at things that are not funny to others. Similar behavior is observed in patients with right hemisphere damage (Brownell & Stringfellow, 2002) that can lead to dementia.
Clearly the existing research shows that dementia can impair humor understanding. However, it is also worth noting that people with dementia can also mask humor misunderstanding. Similarly to depressed individuals (Guendouzi & Muller, 2005; Lindholm, 2008; Lindholm & Wray, 2011; Neville & Byrne, 2009; Whall & Hoes-Gurevich, 1999), those with dementia may camouflage their symptoms with laughter and/or smiling (Hobson, 2019; Lindholm, 2008; Lindholm & Wray, 2011) or by pretending to know the right answer (Matsushita et al., 2017). Saunders et al. (2011) show that humor in cognitively impaired patients may be one of the communicative coping behaviors that empower dementia patients. Lindholm (2008) on the other hand shows that laughter in dementia fits the definition of compensatory behavior utilized to overcome communication barriers and represents a way for the patients to recognize their shortcomings without a more involved verbal display. Laughter is both a way of avoiding revealing problems in language production and comprehension and dealing with those problems without drawing too much attention to them (Lindholm, 2008).
Since the literature shows that humor is enjoyed both by the elderly with dementia and those with depression, it is worth exploring the area further. As the relationship between humor and both of the disorders is rarely discussed together, the present paper aims to fill that gap by addressing three research questions. In our study we firstly wanted to explore how the elderly participants responded to humor. Secondly, we focused on their preferred types of humor. Thirdly, we examined the link between preferred humor type and participants’ disorders (cognitive disorder and depression).
METHODS
The study was conducted in 2019 in the local Geriatrics Clinic. The Clinic admits patients aged 60 plus and offers them a comprehensive geriatric assessment and treatment. The study sample comprised 30 women and 6 men aged from 64 to 94 (average age 80.7, Table 1). All of the participants were in a stable state. Cardiovascular and musculoskeletal disorders dominated among their diagnoses. Elderly participants presented different levels of functional status.
All participants signed an informed consent form prior to the research.
As a first part of the assessment, the elderly participants were tested for both cognitive and depressive symptoms. The following screening scales were used: all patients underwent the Mini Mental State Examination (MMSE) and the Clock Drawing Test as well as the depression assessment with the 15-item Geriatric Depression Scale (GDS). Table 1 presents the results of MMSE and GDS tests as well as demographic statistics.
The participants suspected to have either cognitive decline or depression underwent more detailed tests. The tests included a blood count and a comprehensive metabolic panel (CMP). In addition, head magnetic resonance imaging (MRI)/computer tomography (CT) scans were performed. The scans were followed by a psychological, psychiatric or in some cases neurological consultation. The participants were also tested in terms of functional status using the Katz Index of Independence in Activities of Daily Living (ADL) and Lawton Instrumental Activities of Daily Living scale (IADL). The final dementia/depression diagnosis was based on the results of all the aforementioned screening tests, brain imagining, and consultations according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD10).
The vision and hearing tests (The tests took into account patients’ use of their own glasses and hearing aids) revealed a sufficient level of communication skills. Having taken into account the efficiency of participants’ cognitive functions, the sample was divided into two groups:
- participants without cognitive function impairment, (C0):19 participants
- participants with cognitive function disorders (C1): 7 participants with a mild cognitive impairment (MCI) and 10 participants with dementia
Detailed diagnoses in the dementia group included mainly dementia in Alzheimer disease (F00)- 8 participants, vascular dementia (F01) - 1 participant, fronto-temporal dementia (G31.0) -1 participant.
In total our sample comprised 19 participants without any cognitive dysfunction and 17 participants with some cognitive dysfunction.
Having taken into consideration mood disorders, the study participants were divided into two groups:
- participants without depressive symptoms (D0): 26 participants
- participants with depressive symptoms (D1): 10 participants. This group included participants diagnosed with depressive episode (F32.9) and organic mood disorders (F06.3)
The participants were divided into four groups based on two criteria namely cognitive disorders (MCI/dementia) and mood disorders (depression):
1. Participants without mood or cognitive disorders (healthy participants, P0P0).
2. Participants with cognitive disorder but without mood disorder (P0P1).
3. Participants with mood disorder but without cognitive disorder (P1P0).
4. Patients with both disorders (P1P1).
Table 2 presents statistics regarding elderly participants and their disorders (Please note that all elderly subgroups were small, while the P1P0 group was extremely small, hence we shall treat all results relying on the disorder diagnosis with special caution).
Among those 36 participants 13 had primary education, 7 - basic vocational education, 10 - secondary education and 6 - higher education. We did not find any interaction between education level and disorder type. In Pearson’s Chi-squared test with Yates’ continuity correction we found no statistically significant relationships, when aggregating two lower and two higher educational levels, the results were following - for mood disorder: χ2 (1, N=36)= 0.000, p=1, for cognitive disorder: χ2 (1, N=36)=1.907, p=.167 (Table 3).
The control group comprised 44 students including 2nd year nursing students and 1st year physiotherapy students aged 19 to 48. The students were mostly women (36). There were 7 men and 1 person who did not check the gender box. Out of 44 students, 42 stated their age and the average age of those 42 students was 21.88 years. 39 students answered all test questions, and they were chosen for further statistical analysis.
The study participants were asked to assess the funniness of 40 different examples representing four different groups:
A. verbal containing a linguistic error (10 examples)
B. verbal-visual containing a linguistic error (10 examples)
C. verbal containing a metaphor (10 examples)
D. verbal-visual containing a metaphor (10 examples)
The examples were assessed by giving them a score from 1 to 5 (Likert-like scale with defined two extreme points: 1 - ‘not funny at all’, 5 - ‘very funny’) based on how funny the participant viewed them. We averaged the score for a group of examples, treating the scale as interval (Robitzsch, 2020; Subedi, 2016; Sullivan & Artino, 2013; Wu & Leung, 2017).
All four groups of examples comprising 10 elements each, included 5 humorous and 5 non-humorous items. The humorous items were found on different humorous websites, whereas the non-humorous ones were created by us. The non-humorous examples used the form/style of the humorous ones so that they would resemble them to some extent, except for the funny part. For instance, the following example [1] belongs to the group of verbal containing a linguistic error humor (a typical school joke [School humor in Poland usually involves examples/quotes from children’ s essays or homework]):
[1] Tatuś kupił stary samochód do spółki ze stryjem, którym dojeżdża do pracy/Daddy bought an old car together with an uncle whom he rides to work. (Source: https://www.ciapek.pl/dowcip/tatus-kupil-stary-samochod-do-spolki-ze-stryjem/)
The syntax error makes the sentence illogical, absurd and thus funny (Daddy that rides an uncle to get to work).
Number [2] is a non-humorous example (verbal containing a linguistic error). It contains a similar syntax error to example [1] but is not funny.
[2] The pedestrians with a minute of silence paid tribute to the anniversary who stopped on the streets just like cars and buses (Source: overheard).
Number [3] on the other hand is a verbal-visual humorous example containing a metaphor (Figure 1). The visual part shows a doctor examining his patient’s pocket with a stethoscoe. This leads to a comparison between the physical examination of the patient and the examination of the patient’s finances. The metaphor implies that the doctor is more interested in the patient’s money than his health. It can also be interpreted as an allusion to bribery.
The verbal part of the meme namely: Polska służba zdrowia/Polish healthcare system [3] implies that such a behavior is common in the Polish healthcare system (Source: https://img21.demotywatoryfb.pl//uploads/201604/1460312450_bcgm6n_600.jpg).
Number [4], a non-humorous visual-verbal metaphor-based item, is illustrated by the example below (Figure 2). The visual part presents a doctor whereas the verbal part involves a short metaphor: Szpital to pole bitwy/A hospital is a battlefield [4].
The above items illustrate the four categories/types we focused on in our study’s questionnaire. This can result from: retirement from work, the empty nest syndrome, the increased prevalence of chronic health problems, and the bereavement of a spouse or entry into long-term care (Yang & Victor, 2011). As for the topics of all 40 examples, they were diverse and concerned basic issues of interpersonal relationships, everyday life, health, literature, history, or film. The examples did not require any advanced knowledge on any of the subjects. What is more, the examples that were excluded from our study were the aggressive humor that according to Greengross (2013) is not enjoyed by the elderly. Therefore none of the examples we chose contained foul language, sexual content, drastic or controversial issues.
As for validation procedures for the current experimental stimuli, humorous and non-humorous examples used in the experiment were initially assessed by a group of 8 people (2 humor researchers, 1 geriatrician, 2 students and 3 people over 60).
RESULTS
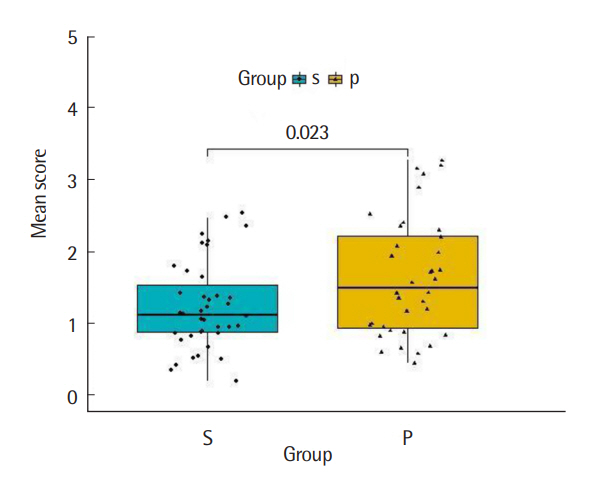
To test the differences in the mean funniness rating between the elderly participants and the control group (the students) we used Welch’s t-test and U Mann-Whitney-Wilcoxon tests. We aggregated results simply by taking the mean of all 40 ratings of a given subject. Figure 3 compares the funniness rating in those two groups. Elderly patients found the examples funnier than the control group according to Welch’s t-test (Delacre, Lakens, & Leys, 2017): t(64.16)=2.33, p=.023. The 95% confidence interval for the effect of the group on the funniness score is between .1 and .7 points. The requirement of approximate normality of both group distributions was met (Anderson-Darling test for normality [Thode, 2002] of the funniness scores show that both groups are approximately normal; students: A(39)= 0.646, p-value=.085, patients: A(36)=0.653, p-value=.081).
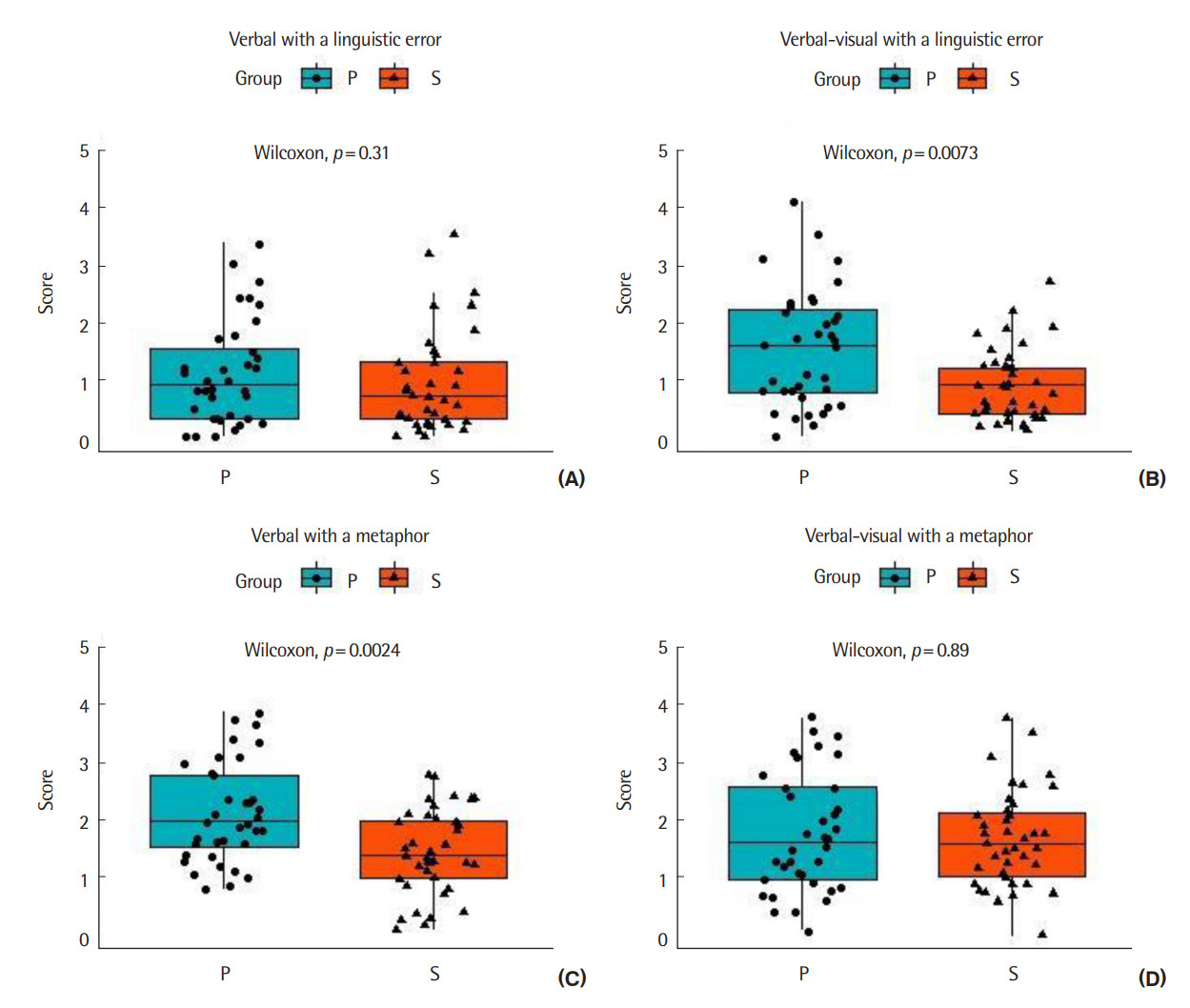
Figure 4 illustrates the results based on the type of the questionnaire examples:
A. verbal containing a linguistic error
B. verbal-visual containing a linguistic error
C. verbal containing a metaphor
D. verbal-visual containing a metaphor
Separate Mann-Whitney comparisons were performed on the 4-dimensional data set, which led to identifying two significant differences (at .01 significance level) (In Anderson-Darling tests we found that several group variables were not approximately normally distributed). There were no significant differences in rating the funniness of the verbal examples containing a linguistic error between the two groups (A type), W (NP=39, Ns=36)=799, p-value=.305. As for the funniness of the verbal-visual examples containing a linguistic error (B type), we noticed statistically significant differences, W=955, p=.007. Taking into account distribution shapes (Fig. 4B), we might have assumed that elderly participants (Mdn=1.6, large Ra=4.1) found those examples funnier than the control group (Mdn=0.9, small Ra=2.6), with common language effect size f=68% (McGraw & Wong 1992) (Two-thirds of sample pairs supported the superiority of patient comicality scores). It seemed that error-based examples were seen as funnier by the elderly participants when accompanied by a visual part (image). As for the metaphor-based examples (C type) we also noticed statistically significant differences in comicality scores, W=988, p=.002. Because boxplots for the two groups looked very similar (Figure 4C), we interpreted the results as the proof for the simple shift difference. The patients (Mdn=2.0) found verbal examples containing metaphor (without image) funnier than the control group (Mdn=1.4), with common language effect size f=70%. On the other hand, the verbal-visual examples containing metaphor (D type) were rated likewise by the patients and the control group and no difference was found, W=716, p=.89.
We further investigated differences in comicality scores by splitting the group of elderly participants according to their diagnosis. Figure 5 illustrates the differences in the funniness rating of the four types of examples (A-D) between the participants and the control group.
We compared each subgroup of elderly participants directly to the control group with the use of the non-parametric U Mann-Whitney-Wilcoxon test. Table 4 provides the Wilcoxon W statistic together with test p-values with Benjamini-Hochberg correction for multiple comparisons (false discovery ratio, FDR - Benjamini & Hochberg, 1995). To assess the shift in median in the case of statistically significant differences, we inspected boxplots, as well as calculated bootstrap percentile confidence intervals, at 5% or 10% significance level, with 10,000 repetitions (Rousselet, Pernet, & Wilcox, 2021, see again Table 4 for details).
There are no significant differences in the perceived funniness of the verbal error-based examples (type A) between participants and students. The same is true for verbal-visual examples with a metaphor (type D); though the least healthy group (P1P1, MdnP1P1=0.8) might have enjoyed this humor type less than students (MdnS=1.6), W (Ns=39, NP1P1=8)=235, p=.026, FDR corrected pBH-value <0.1, common language effect size f=75%, 90% bootstrap CI [-0.1, -1.1] for the difference (Table 4). Still significant discrepancies were found among participants considering verbal-visual examples with a linguistic error (Table 4B), and verbal examples with a metaphor (C). Participants with sole cognitive disorder (P0P1) seemed to be pleased with both types of humor most, more than students (FDR corrected pBH-values<0.05, Table 4). Healthy participants (P0P0) laughed at verbal-metaphor examples more than control subjects (C type, pBH <0.05) in which they resembled cognitive disorder participants (P0P1), but behaved similarly to students when exposed to verbal-visual-error examples. Participants with depression (P1P0) acted the opposite. They did not enjoy metaphor at all (C and D example types), while still were able to appreciate verbal-visual examples with a linguistic error (type B, pBH <0.1).
DISCUSSION & CONCLUSION
This study aimed to investigate the humor preferences in elderly patients with cognitive disorder, depression or both disorders. The study’s key results form three distinctive groups: participants’ overall response to the humor, their preferred types of humor, and the relationship between preferred humor type and participants’ disorders.
As for the overall response to humor, the elderly participants found both humorous and non-humorous examples funnier than the control group. This can be explained by a number of factors. Firstly, according to the study by Shammi and Stuss (2003), elders appreciate humor more than young people. In their study, healthy elders perceived both humorous and neutral statements as funnier than the young adults. This difference was not due to lack of understanding of the jokes, as the elderly were able to differentiate between the humor and the neutral statements just as the young subjects did, showed no slowness in emotional response to the jokes, and actually enjoyed the humor more than the young group.
Secondly, even elders with dementia or depression are still able to understand and appreciate some humor (Clark et al., 2015; Clark et al., 2016; Shammi & Stuss, 1999; Walter et al., 2007). Perhaps this can be explained by older adults being equipped with enhanced attentional bias for positive stimuli (Meng et al., 2015). This can also explain why some patients in our study found nonhumorous examples funny. Alternatively, laughing at things that are not funny to others can be attributed to some types of dementia or neurological disorder, e.g. right temporal variant frontotemporal dementia (rtvFTD) (Wong & Kumfor, 2022), right hemisphere damage (Brownell & Stringfellow, 2002), behavioral variant frontotemporal dementia (bvFTD), or semantic dementia (SD) (Clark et al., 2015). Thirdly, it is worth considering a social factor, such as interactions with students that the patients really enjoyed. Some of the patients were so engaged that they kept asking students whether the students would be graded for the questionnaires. According to Preston, Marshall, and Bucks (2007) humor can help people with dementia to create a point of contact or shared experience. The elderly take part in research projects because they treat them as an opportunity to socialize (Jacelon, 2007) or reduce their sense of social loneliness (Schiau, 2016).
According to Yang and Victor (2011) the prevalence of loneliness increases with age. This can result from retirement from work, the empty nest syndrome, the increased prevalence of chronic health problems, and the bereavement of a spouse or entry into long-term care (Yang & Victor, 2011). Hospitalization may lead to decreased functional capacity, physical weakness and emotional instability as the hospital is permeated by stressors that interfere with well-being (Rosa et al., 2018). Humor used by patients, on the other hand, can improve their hospital experience (Haydon, van der Reit, & Browne, 2015). It has been shown that even patients with severe Alzheimer’s use humor in their communication with medical personnel (Moos, 2011).
Lastly, the patients knew the purpose of the questionnaire and thus may have wanted to show off their sense of humor. This may be linked to humor being a socially desirable quality (Billig, 2007). The willingness to show off, the desire to help students and highrated funniness of the examples in the questionnaire can all be explained by a higher social desirability and acquiescence among older people (Vigil-Colet, Morales-Vives, & Lorenzo-Seva, 2013).
With regard to the preferred types of humor in the geriatric patients, our study shows that out of four types of humor, geriatric patients rated two types higher than the control group. Those two funniest types were the visual error-based jokes and non-visual metaphor-based jokes. Those two types of humor were the easiest to understand for several reasons.
Firstly, the visual part of the error-based jokes illustrated some simple elements mentioned in the verbal part, e.g., the image of a hare illustrated the joke about the hare. Finding error-based jokes funny is in line with the study by Bischetti et al. (2019) that shows that older adults find linguistic error-based jokes easier to understand. As for metaphor-based humor, the jokes presented to the patients could be classified as well-known or uninteresting jokes. The patients may have heard them before, which implies that their understanding did not require much of a cognitive effort. Perhaps older people, in general, enjoy familiar humor due to the satisfaction coming from remembering the joke and not necessarily because it is complex and surprising (Suls, 1975). Alternatively, it can be explained by the fact that with age cognitive ability and humor comprehension decline, leading to an increased appreciation of the humor as the joke requires more cognitive effort from the individual (Schaier & Cicirelli, 1976). The question remains if all jokes require more cognitive effort, even those that are particularly simple. Which jokes are appreciated may depend not just on their complexity level but also their content (Holland, 1982; Libera, 2020; Lynch 2010; Plester & Inkson, 2019).
Clark et al. (2015) show that familiar humor is easier to understand by the patients with a behavioral variant of frontotemporal dementia (bvFTD) whereas novel humor is found difficult to detect. In our study we did not investigate different types of dementia, and thus cannot confirm the link between familiar humor and a behavioral variant of frontotemporal dementia. However, our results confirm that familiarity plays an important role in both humor appreciation (Goldstein 1970; Goldstein et al., 1972; Suls 1975; Triezenberg, 2004;) and dementia care (Son et al., 2002). Since familiar humor may lessen the tension caused by its novelty and thus make a person enjoy it more (Goldstein, 1970), we can assume that familiar jokes may be particularly appreciated by dementia patients.
Regarding the results of the relationship between preferred humor type and participants’ disorders, among four sample subgroups, the patients with a single disorder rated the funniness of the examples highest. It may have resulted from the patients’ desire to show off in a social situation or from their ability to appreciate the positive side of the illness being not severe enough to exclude them from the social life.
Both cognitive decline and depression may be of different severity. Diseases that are mild or at an early stage are characterized by high self-awareness and thus ability to camouflage/mask the symptoms as in the case of an early- stage Alzheimer (Stein-Parbury, 2014), mild yet chronic depression (Westerbeek, Meeuwesen, Brinkgreve, & Gomperts, 2014) or mild dementia (Hobson, 2019). In our study the majority of participants had mild dementia / mild cognitive impairment (MCI) and mild depression. We selected those patients who were capable of fully participating in our study.
Mild cognitive impairment (MCI) has been characterized as an intermediate state of cognitive function between the changes seen in aging and those fulfilling the criteria for dementia. MCI criteria include cognitive decline, but activities are intact, except perhaps for some mild inefficiencies (Petersen, 2011). Whereas dementia is a syndrome - usually of a chronic or progressive nature - in which there is deterioration in cognitive function (i.e., the ability to process thought) beyond what might be expected from normal ageing which is sufficient to impair functional status (i.e., activities of daily living) (WHO, 2020).
The literature on the subject shows that people with dementia or late -life depression may mask the symptoms of their disease using, among others methods, laughter and/or smiles (Guendouzi & Muller, 2005; Lindholm, 2008; Lindholm & Wray, 2011; Neville & Byrne, 2009; Whall & Hoes-Gurevich, 1999). In the case of dementia participants, the questionnaire or perhaps the social interaction with students may have been ‘the pleasant stimuli’ that dementia participants ‘reacted to with laughter and smile’ (Takeda et al., 2010). As for depression, older people minimize their depressed mood to others (Kortebein & Means, 2012) and may be more successful than their younger counterparts at masking or hiding symptoms of depression (Papas, Niessen, & Chauncey, 1991). Similar results of the participants with a single disorder can be also explained by dementia and late-life depression being often correlated or hard to distinguish (Leyhe et al., 2017; Steffens & Potter, 2008; Steinberg & Rosenberg, 2017).
The results on humor perception in people with a single or both disorders are surprising. Out of all patients with a single disorder, those with cognitive disorders rated jokes slightly higher than those with depression. This can be explained by dementia and MCI patients trying to camouflage their cognitive decline, e.g., by pretending to know the right answer (Matsushita et al., 2017). Alternatively, it can be the result of a characteristic for Alzheimer’s disease: greater empathy and mimicking the emotions of people around (Sturm et al., 2013).
Our study shows humor can be understood and enjoyed by patients with mild depression and dementia. It may be surprising that humorous metaphors were comprehended by the participants with dementia since dementia or Alzheimer patients are more likely to have comprehension problems with metaphors (Fujimoto, Nakamura, Tsuda, Wakutani, & Takao, 2019). However, Papagno (2001) proves non-literal language is a relatively preserved function in very mild Alzheimer’s disease patients.
Further research could explore whether patients who have similar language comprehension issues to those with dementia fully understand and enjoy metaphor -based humor. Identifying what types of metaphors different patients find amusing could both facilitate diagnosis and help select humor that amuses them. Understandable humor (familiar and simple) could be used in their therapy to boost their mood, enhance their communication, and improve relationships.
The healthy participants and those with both disorders performed similarly to the students. Only a few jokes were rated higher by the healthy patients than by the students and only a few were rated lower by the patients with both disorders in comparison to the students. However, it was statistically insignificant. Those similar results can indicate that what people find funny is age-independent. Alternatively, it can prove that the perceived funniness of persons with a single disorder may be a result of them using humor as a coping mechanism. Such a coping mechanism no longer works in the case of coexisting dementia and depression. The occurrence of both disorders in older people lessens their compensatory abilities and hinders their reaction in both social interaction and in response to different stress factors (Kobayashi & Kato, 2011).
Limitations
Our study has several limitations. Firstly, due to the small sample used in the study, it is difficult to generalize the humor preferences of all older people with cognitive disorder and/or depression. Nevertheless, this study can serve as a starting point for comparing humor preferences in those particular groups of patients. Also, with a greater number of participants it would have been difficult to allocate an hour or more for each questionnaire. The advantage of a small sample was the quality of the interaction with the participants. The patients took as much time as they needed to answer the questions. In order to facilitate the completion of questionnaires, the questions were read out loud to some of the study participants (and repeated on request) and their answers were written down by the students. Another issue related to our sample was an uneven number of women and men. For that reason, we avoided any gender-related interpretations of our findings.
Secondly, in our study we focused on age-related humor inhibitors whereas future studies could focus both on age-related humor inhibitors (diseases) and facilitators such as experience of using humor throughout life as suggested by Wanzer, Sparks, and Frymier (2009).
Thirdly, exploring humor and the correlation between different types of dementia and levels of depression in the elderly could provide a fuller picture of changing humor preferences as the disorders progress.
Fourthly, humor is such a subjective phenomenon (Latta, 2011) that it is difficult to select universally funny jokes for one age group, let alone for both generations. However, in our study we tried to balance error-based jokes with metaphor-based jokes and visual components with the verbal ones. Doing so we wanted to appeal both to elders (more ‘verbal humor’ generation) and youngsters (more ‘visual humor’ generation).
Finally, this study focused on verbal humor only whereas nonverbal humor is also enjoyed by the elderly with dementia (Baumgartner & Renner, 2019). Future research could explore the differences in preferences between verbal and non-verbal humor as well as specific.